Innovation
Technologically assisted Surgical Innovation is the path to improve patient outcomes
The foundation firmly believes that disciplined surgical innovation is the hallmark of the progress of surgical sciences. Our FastTrack innovation spiral followed Idea, Development, Exploration, Assessment and Long-term study (IDEAL): the scientific framework designed at Oxford University to develop new surgical procedures which are safe, reproducible and with benchmarks for patient outcomes. Our surgical innovation pipeline passed through a global network of Vattikuti co-branded institutions, leveraging their strengths for obtaining proof of concept and its ultimate application on human subjects weaving a fool-proof patient safety net. For each surgical innovation we handpicked subject related, skilled surgical masters from across the globe.
In the recent past, we invested in developing Robotic Kidney Transplant Kidney Surgery and Menon Precision Prostatectomy (MPP) which are disruptive and fast approaching to be the standard of care.
Robotic Kidney Transplant
under Regional Hypothermia
The technique of robotic kidney transplant was successfully implemented in 2013 in India, by a team of experts from India and United States at the Medanta Institute of Robotic Surgery, Medanta Medicity Gurugram and the Institute of Kidney Diseases Research Center (IKDRC) Ahmedabad. Since then it has been successfully adopted globally. The foundation supported the development of the procedure and trained the surgeons for it’s safe implementation.
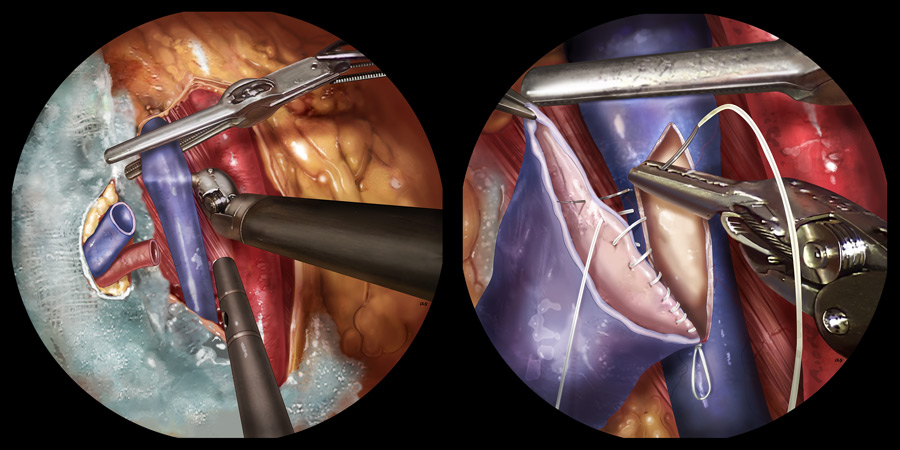
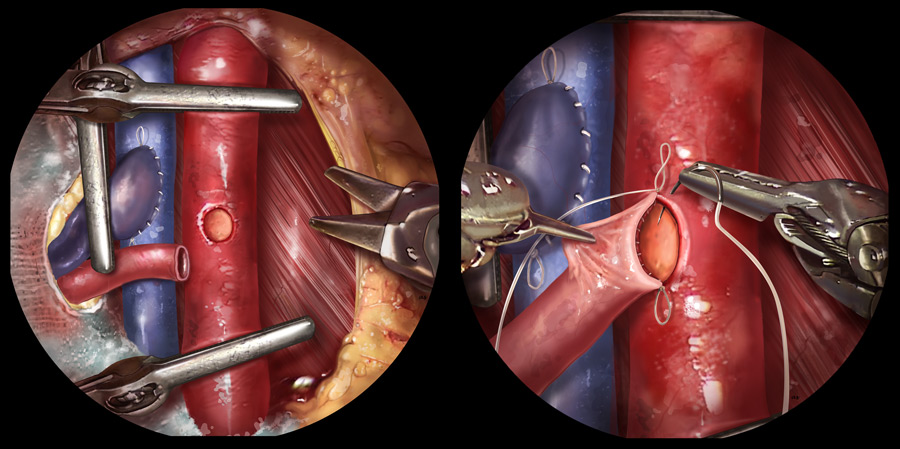
The procedure was conceived and developed at our flagship, the Vattikuti Urology Institute, Henry Ford Hospital including the technique to keep the kidney sufficiently cool to allow time for the team to complete high quality vascular anastomosis and join the donor kidney to the body of the recipient. The proof of the concept was obtained on the fresh cadavers at the Ohio State University, Columbus Ohio. Subsequently, the foundation facilitated the training of the surgeons by taking teams of the surgeons to India and sending the expert surgeons to other centers for smooth adoption of the procedure at different institutions in India, United States, Europe and London.
Robotic Transplant Program Across the Globe
This video is age-restricted
As of June 2021, ~2000 transplants have been performed at 48 Centers in India, United State, Europe, London and other Asian Countries. with significant improvement in short and long-term patient outcomes. Published literature confirms high patient acceptance, significant reduction of pain and use of painkillers in the postoperative period. It has wiped out lymphoceles and wound infections, two serious postoperative complications of conventional kidney transplant recipient surgery
Seminal Publications on Robotic Kidney Transplantation with Regional Hypothermia from the Vattikuti network of Institutions
Robotic Kidney Transplantation with Regional Hypothermia versus Open Kidney Transplantation for Patients with End Stage Renal Disease: An Ideal Stage 2B Study.
Ahlawat R, Sood A, Jeong W, Ghosh P, Keeley J, Abdollah F, Kher V, Olson P, Farah G, Wurst H, Bhandari M, Menon M.
J Urol. 2021 Feb;205(2):595-602. doi: 10.1097/JU.0000000000001368. Epub 2020 Sep 16. PMID: 329
Learning Curves and Timing of Surgical Trials: Robotic Kidney Transplantation with Regional Hypothermia.
Ahlawat RK, Tugcu V, Arora S, Wong P, Sood A, Jeong W, Bhandari M, Menon M.
J Endourol. 2018 Dec;32(12):1160-1165. doi: 10.1089/end.2017.0697. Epub 2018 Apr 26. PMID: 29587531 4110
Response to Barry re: Learning Curves and Timing of Surgical Trials: Robotic Kidney Transplantation with Regional Hypothermia by Ahlawat et al. (From: Barry JM. J Endourolo 2018;32:1166; DOI: 1089/end.2018.0419).
Arora S, Sood A, Wong P, Ahlawat R, Menon M.
J Endourol. 2018 Dec;32(12):1167. doi: 10.1089/end.2018.29046.sar. Epub 2018 Nov 8. PMID: 30280919 No abstract available.
Robotic kidney transplantation: current status and future perspectives.
Territo A, Mottrie A, Abaza R, Rogers C, Menon M, Bhandari M, Ahlawat R, Breda A.
Minerva Urol Nefrol. 2017 Feb;69(1):5-13. doi: 10.23736/S0393-2249.16.02856-3. Epub 2016 Nov 30. PMID: 28009142
Ontogeny of a surgical technique: Robotic kidney transplantation with regional hypothermia
Sood A, McCulloch P, Dahm P, Ahlawat R, Jeong W, Bhandari M, Menon M.
Int J Surg. 2016 Jan;25:158-61. doi: 10.1016/j.ijsu.2015.12.061. Epub 2015 Dec 21. PMID: 26718609
Minimally invasive kidney transplantation: perioperative considerations and key 6-month outcomes.
Sood A, Ghosh P, Jeong W, Khanna S, Das J, Bhandari M, Kher V, Ahlawat R, Menon M.
Transplantation. 2015 Feb;99(2):316-23. doi: 10.1097/TP.0000000000000590. PMID: 25606784
Minimally invasive renal autotransplantation.
Sood A, Jeong W, Ahlawat R, Abdollah F, Sammon JD, Bhandari M, Menon M.
J Surg Oncol. 2015 Dec;112(7):717-22. doi: 10.1002/jso.23939. Epub 2015 May 20. PMID: 25995142 .
Robotic renal transplantation: Current status.
Sood A, Ghosh P, Menon M, Jeong W, Bhandari M, Ahlawat R.
J Minim Access Surg. 2015 Jan-Mar;11(1):35-9. doi: 10.4103/0972-9941.147683. PMID: 25598597
The growth of computer-assisted (robotic) surgery in urology 2000-2014: The role of Asian surgeons.
Dalela D, Ahlawat R, Sood A, Jeong W, Bhandari M, Menon M.
Asian J Urol. 2015 Jan;2(1):1-10. doi: 10.1016/j.ajur.2014.09.010. Epub 2015 Apr 16. PMID: 29264114 Free PMC article.
Reply to Jyotirmoy Das, Sudhir Kumar, Sangeeta Khanna, and Yatin Mehta's letter to the editor re: Mani Menon, Akshay Sood, Mahendra Bhandari, et al. Robotic kidney transplantation with regional hypothermia: a step-by-step description of the Vattikuti Urology Institute-Medanta Technique (IDEAL Phase 2a). Eur Urol 2014;65:991-1000: robotic kidney transplantation: cool the kidney, warm the patient.
Ahlawat R, Balakrishnan G, Kher V, Menon M.
Eur Urol. 2014 Jun;65(6):e88. doi: 10.1016/j.eururo.2014.02.007. Epub 2014 Feb 15. PMID: 24589331 No abstract available.
Robotic kidney transplantation with intraoperative regional hypothermia.
Abaza R, Ghani KR, Sood A, Ahlawat R, Kumar RK, Jeong W, Bhandari M, Kher V, Menon M.
BJU Int. 2014 Apr;113(4):679-81. doi: 10.1111/bju.12572. PMID: 24238345
Robotic kidney transplantation with regional hypothermia: a step-by-step description of the Vattikuti Urology Institute-Medanta technique (IDEAL phase 2a).
Menon M, Sood A, Bhandari M, Kher V, Ghosh P, Abaza R, Jeong W, Ghani KR, Kumar RK, Modi P, Ahlawat R.
Eur Urol. 2014 May;65(5):991-1000. doi: 10.1016/j.eururo.2013.12.006. Epub 2013 Dec 19. PMID: 24388099 Clinical Trial.
Robotic kidney transplantation with regional hypothermia: evolution of a novel procedure utilizing the IDEAL guidelines (IDEAL phase 0 and 1).
Menon M, Abaza R, Sood A, Ahlawat R, Ghani KR, Jeong W, Kher V, Kumar RK, Bhandari M.
Eur Urol. 2014 May;65(5):1001-9. doi: 10.1016/j.eururo.2013.11.011. Epub 2013 Nov 20. PMID: 24287316.
Application of the statistical process control method for prospective patient safety monitoring during the learning phase: robotic kidney transplantation with regional hypothermia (IDEAL phase 2a-b).
Sood A, Ghani KR, Ahlawat R, Modi P, Abaza R, Jeong W, Sammon JD, Diaz M, Kher V, Menon M, Bhandari M.
Eur Urol. 2014 Aug;66(2):371-8. doi: 10.1016/j.eururo.2014.02.055. Epub 2014 Mar 4. PMID: 24631408